Study design and population
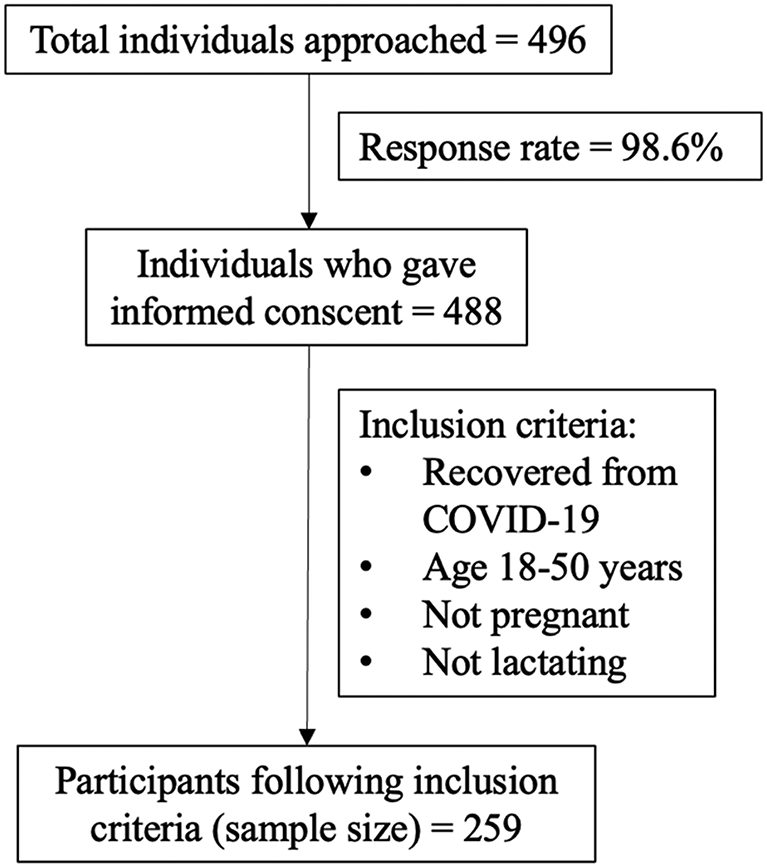
A cross-sectional survey was conducted to collect retrospective data from the recovered cases of COVID-19 in Pakistan. The target population was adults aged 18–50 years. Pregnant and lactating females were excluded due to their special dietary considerations and health practices while older adults were excluded due to their potential recall difficulties. Data were collected using a self-administered online questionnaire generated on Google Forms and disseminated via email and social media platforms. Google Forms had two levels of response-based proceeding to subsequent sections. First was the consent to participate in the study after reviewing the participant statement. If the participant declined to take part in the study, the questionnaire ended at that point, and no data was collected. Second was after collecting the socio-demographic information to see if the participants had suffered from COVID-19 in the past or not. The questionnaire ended for those who did not suffer from COVID-19, and hence, the purposive sampling technique was used to collect further information only from the recovered cases of COVID-19. The sample size was calculated to be 259 from the total number of recovered cases of COVID-19 in Pakistan in March 2020 [16], using the Kish Leslie formula [17] with a 95% confidence level and 5% precision level.
$$\:n=\frac{{Z}^{2}\times\:\:p\times\:(1-p)}{{E}^{2}}$$
496 people were contacted before we could reach the calculated sample size of eligible participants. After achieving the calculated sample size, a further survey was stopped. A summary of the sampling process is given in Fig. 1.
Sociodemographic characteristics
Sociodemographic information included age (years), gender, weight (kilograms), height (feet and inches), and employment status (employed/unemployed). Body mass index (BMI) was calculated using the self-reported weight and height.
Dietary practices
Adherence to the Pakistan Dietary Guidelines for Better Nutrition (PDGN) was used as a tool to access the dietary practices of study participants. According to the PDGN recommendations prepared by the Planning Commission of Pakistan [18], there must be 4–5 servings of grains and cereals per day and 2–3 servings of meat and pulses, vegetables, fruits, and milk/milk products per day. The questionnaire was developed from the guidelines, and five close-ended questions based on each PDGN recommendation were included. If the individual answered “yes” to following a recommendation, a score of 1 was given, and 0 scores if answered “no.” Adherence to the dietary guidelines was measured on a scale of 0 (not following any recommendation) to 5 (following all five recommendations). Two mean scores were calculated to indicate the dietary practices pre- and post-COVID-19 infection. Change in the dietary practices (Δ dietary adherence score) was calculated by subtracting the dietary adherence score after the infection from the score before the infection.
Health practices
To access the health practices of study participants, Breslow’s seven health practice scores (BHPS) [19] were used. The BHPS measures participants’ adherence to seven good health practices, which include never smoking cigarettes, regular physical activity, maintaining proper weight, moderate or no use of alcohol, 7–8 h of sleep per day regularly, eating breakfast, and not eating between meals. Keeping in view the religious and sociocultural concerns of the study population, questions regarding alcohol consumption were omitted from the questionnaire. The questionnaire included six close-ended questions based on each health practice. If the individual answered “yes” to following a practice, a score of 1 was given, and a 0 score if answered “no.” Adherence to the health practices was calculated on a scale of 0 (not following any good health practices) to 6 (following all six good health practices). Two mean scores were calculated to indicate the health practices pre- and post-COVID-19 infection. Change in the health practices (Δ health practices score) was calculated by subtracting the health practices score after the infection from the score before the infection.
Food choice motives
To access the motives behind the food choices before and after suffering from COVID-19, the Food Choice Questionnaire (FCQ) developed by Steptoe, Pollard [20] was used. The original version of the questionnaire includes 36 items that are divided into nine subscales, including health (6 items), mood (6 items), convenience (5 items), sensory appeal (4 items), natural content (3 items), price (3 items), weight control (3 items), familiarity (3 items) and ethical concern (3 items). Participants were asked to rate every item on a scale of 1 to 4, where 1 = Not at all important; 2 = A little important; 3 = Moderately important; 4 = Very important. Two scores were calculated for each subscale by calculating the average of the rating of individual items, indicating the food choice motives pre- and post-COVID-19 infection. Change in the importance of food choice motives (Δ Convenience, Δ Health, Δ Mood, Δ Sensory appeal, Δ Natural content, Δ Price, Δ Weight control, Δ Familiarity, and Δ Ethical concern) was calculated by subtracting the score for each motive after the infection from the score before the infection.
Statistical analysis
Statistical analysis was performed using Statistical Package for Social Sciences (SPSS) version 25. The level of significance was set at p = 0.05. Shapiro-Wilk test was used to analyze the normality of data. Data was found to be non-parametric. McNemar’s test and Wilcoxon sign ranked test were used to determine the statistically significant change in the dietary practices, health practices, and food choice motives scores pre- and post-COVID-19 infection. Spearman correlation was used to study the relation between the changes in dietary practices, health practices, and food choice motives. Multiple linear regression was used to study the effect of changes in food choice motives (predictor variable) on the dietary and health practices (outcome variable) pre- and post-COVID-19 infection.
Ethical approval
This study was approved by the Institutional Review Committee for Biomedical Research at the University of Veterinary and Animal Science, Lahore, Pakistan (approval number: 125/IRC/BMR). The committee reviewed and approved the participant statement. Informed consent was sought from participants before the data collection. For data protection, all the responses were anonymized by the principal investigator. Personal information, including the name and email address, were removed from the data before handling to maintain confidentiality.

